

Abstract

Introduction: The optimal clinical setting and cell product characteristics for chimeric antigen receptor (CAR) T cell therapy in multiple myeloma (MM) are uncertain. In CLL patients treated with anti-CD19 CAR T cells (CART19), prevalence of an early memory (early-mem) T cell phenotype (CD27+ CD45RO- CD8+) at time of leukapheresis was predictive of clinical response independently of other patient- or disease-specific factors and was associated with enhanced capacity for in vitro T cell expansion and CD19-responsive activation (Fraietta et al. Nat Med 2018). T cell fitness is therefore a major determinant of response to CAR T cell therapy. In an accompanying abstract (Cohen et al.), we report that higher percentage of early-mem T cells and CD4/CD8 ratio within the leukapheresis product are associated with favorable clinical response to anti-BCMA CAR T cells (CART-BCMA) in relapsed/refractory MM. Here, we compare leukapheresis samples from MM patients obtained at completion of induction therapy (post-ind) with those obtained in relapsed/refractory (rel/ref) patients for frequency of early-mem T cells, CD4/CD8 ratio, and in vitro T cell expansion.
Methods: Cryopreserved leukapheresis samples were analyzed for the percentage of early-mem T cells and CD4/CD8 ratio by flow cytometry and in vitro expansion kinetics during anti-CD3/anti-CD28 bead stimulation. Post-ind samples were obtained between 2007 and 2014 from previously reported MM trials in which ex-vivo-expanded autologous T cells were infused post-ASCT to facilitate immune reconstitution (NCT01245673, NCT01426828, NCT00046852); rel/ref samples were from MM patients treated in a phase-one study of CART-BCMA (NCT02546167).
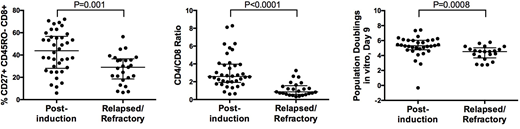
Results: The post-ind cohort includes 38 patients with median age 55y (range 41-68) and prior exposure to lenalidomide (22), bortezomib (21), dexamethasone (38), cyclophosphamide (8), vincristine (2), thalidomide (8), and doxorubicin (4); median time from first systemic therapy to leukapheresis was 152 days (range 53-1886) with a median of 1 prior line of therapy (range 1-4). The rel/ref cohort included 25 patients with median age 58y (range 44-75), median 7 prior lines of therapy (range 3-13), and previously exposed to lenalidomide (25), bortezomib (25), pomalidomide (23), carfilzomib/oprozomib (24), daratumumab (19), cyclophosphamide (25), autologous SCT (23), allogeneic SCT (1), and anti-PD1 (7). Median marrow plasma cell content at leukapheresis was lower in the post-ind cohort (12.5%, range 0-80, n=37) compared to the rel/ref cohort (65%, range 0-95%). Percentage of early-mem T cells was higher in the post-ind vs rel/ref cohort (median 43.9% vs 29.0%, p=0.001, left figure). Likewise, CD4/CD8 ratio was higher in the post-ind vs rel/ref cohort (median 2.6 vs 0.87, p<0.0001, mid figure). Magnitude of in vitro T cell expansion during manufacturing (measured as population doublings by day 9, or PDL9), which correlated with response to CART19 in CLL, was higher in post-ind vs rel/ref cohort (median PDL9 5.3 vs 4.5, p=0.0008, right figure). Pooling data from both cohorts, PDL9 correlated with both early-mem T cell percentage (Spearman's rho 0.38, multiplicity adjusted p=0.01) and CD4/CD8 ratio (Spearman's rho 0.42, multiplicity adjusted p=0.005). Within the post-ind cohort, there was no significant association between early-mem T cell percentage and time since MM diagnosis, duration of therapy, exposure to specific therapies (including cyclophosphamide, bortezomib, or lenalidomide), or bone marrow plasma cell content at time of apheresis. However, in the post-ind cohort, there was a trend of toward lower percentage early-mem phenotype (29% vs 49%, p=0.07) and lower CD4/CD8 ratio (median 1.4 vs 2.7, p=0.04) among patients who required >2 lines of therapy prior to apheresis (n=3) compared to the rest of the cohort (n=35).
Conclusion: In MM patients, frequency of the early-mem T cell phenotype, a functionally validated biomarker of fitness for CAR T cell manufacturing, was significantly higher in leukapheresis products obtained after induction therapy compared to the relapsed/refractory setting, as was CD4/CD8 ratio and magnitude of in vitro T cell expansion. This result suggests that CAR T cells for MM would yield better clinical responses at early points in the disease course, at periods of relatively low disease burden and before exposure to multiple lines of therapy.
Garfall:Novartis: Research Funding; Kite Pharma: Consultancy; Amgen: Research Funding; Bioinvent: Research Funding. Cohen:GlaxoSmithKline: Consultancy, Research Funding; Kite Pharma: Consultancy; Oncopeptides: Consultancy; Celgene: Consultancy; Novartis: Research Funding; Poseida Therapeutics, Inc.: Research Funding; Bristol Meyers Squibb: Consultancy, Research Funding; Janssen: Consultancy; Seattle Genetics: Consultancy. Fraietta:Novartis: Patents & Royalties: WO/2015/157252, WO/2016/164580, WO/2017/049166. Davis:Novartis Institutes for Biomedical Research, Inc.: Patents & Royalties. Levine:CRC Oncology: Consultancy; Brammer Bio: Consultancy; Cure Genetics: Consultancy; Incysus: Consultancy; Novartis: Consultancy, Patents & Royalties, Research Funding; Tmunity Therapeutics: Equity Ownership, Research Funding. Siegel:Novartis: Research Funding. Stadtmauer:Janssen: Consultancy; Amgen: Consultancy; Takeda: Consultancy; Celgene: Consultancy; AbbVie, Inc: Research Funding. Vogl:Karyopharm Therapeutics: Consultancy. Milone:Novartis: Patents & Royalties. June:Tmunity Therapeutics: Equity Ownership, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties, Research Funding; Tmunity Therapeutics: Equity Ownership, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties, Research Funding; Immune Design: Membership on an entity's Board of Directors or advisory committees; Novartis Pharmaceutical Corporation: Patents & Royalties, Research Funding; Celldex: Consultancy, Membership on an entity's Board of Directors or advisory committees; Immune Design: Membership on an entity's Board of Directors or advisory committees; Novartis Pharmaceutical Corporation: Patents & Royalties, Research Funding. Melenhorst:Novartis: Patents & Royalties, Research Funding; Incyte: Research Funding; Tmunity: Research Funding; Shanghai UNICAR Therapy, Inc: Consultancy; CASI Pharmaceuticals: Consultancy.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal